
ALZHEIMER’S DISEASE (AD) may be in your future, but you can head it off! A person must be proactive rather than reactive to prevent this devastating disease. After its onset, it is too late to reverse this most common form of dementia. It is an incurable, degenerative, and terminal disease which was first described by the German psychiatrist and neuro-pathologist, Alois Alzheimer in 1906 and was subsequently named after him. Generally, it is diagnosed in people over 65 years of age, although the less-prevalent “early-onset” of Alzheimer's does occur before this age. In 2011, there were 36 million sufferers in the US. Alzheimer's is predicted to affect 1 in 3 over the age of 65. By 2050, half of all people over the age of 80 are predicted to have it! Medical science already has the tools to prevent it, but very few Doctors know about them, let alone make their recommendation.
The risk factors for AD includes family history, gluten intolerance, heavy metal excess, fever blisters, glucose intolerance, obesity, head trauma, drug, age, physical and psychological stress. Stress can not only be diagnosed, but quantified by a simple office test: Heart Rate Variation (HRV). Also, if one has a single gene Apo E4 there is a 75% chance and if a double E4 a 94% chance of the disease.
The earliest observable symptoms are often mistakenly thought to be “age-related” senior moments. The inability to acquire new memories, the difficulty in recalling recently observed facts are noted first by the individual, then by loved ones and lastly by friends. These individuals, particularly those with a high social IQ, cover up these mental lapses with believable excuses. As the disease advances, symptoms include confusion, irritability, aggression, mood swings, language breakdown, long-term memory loss and the general withdrawal of the sufferer as their senses decline. Gradually, bodily functions are lost, ultimately leading to death. Individual prognosis is difficult to assess, as the duration of the disease varies. AD develops for an indeterminate period of time before becoming fully apparent, and it can progress undiagnosed for years. The mean life expectancy following diagnosis is approximately seven years. Fewer than three percent of individuals live more than fourteen years after diagnosis. When AD is suspected, the diagnosis is usually confirmed with behavioral assessments and cognitive tests, such as a MMSE. A Psychological Inventory Test (to be covered in a later posting) that checks nine different brain areas of function also helps in diagnosis and prognosis. It is best to pick up the disease in its earliest stages when much can be done to delay or even prevent it. Often I will order a MRI to look at the hippocampus volume, and if in real doubt do a PET scan with a PIB contrast.
If Alzheimer’s is in your future, much can be done to greatly delay, or better yet, prevent it. Despite the many ways to determine if you are in harms way, there is no guarantee that it will arrive until after it is too late. Therefore, an ounce of prevention should be considered before a ton of care. One cannot change their genes (Apo E or Family History), but can certainly amend them in what is now termed epigenetic modification. The research indicates that AD is mainly an inflammatory process albeit a slow ongoing oxidative smoldering process. Involved in this process are two key moleules, Nrf2 and BDNF. Nrf2 is a master regulator molecule of the antioxidant response. This response is important to diminish our oxidative stressors. Because Nrf2 is able to induce genes important in combating oxidative stress, it activates the body’s own protective response, Nrf2 is able to protect from a variety of oxidative stress-related complications, even in situations where the administration of exogenous antioxidants (such as Vitamin C and Vitamin E) have failed. The other important player, BDNF keeps nerve cells alive and stimulaes the growth of new ones. Recent studies shows that it prevents and reverse Alzheimer’s independent of the amyloid plaque tangles. BDNF levels can be naturally boosted by heavy exercise and caloric restriction. Nutrients that also help make BDNF or protect it from declining are acetyl-l-carnitine, fish oil, blueberries, and curcumin.
There are both prescription drugs and supplements that are recommended for AD. The three drugs that are FDA approved to increase an important chemical in neuro-transmission, Acetyl Choline, are Aricept, Exelon and Razadyne. The other FDA medication is Nemanda which tries, but not completely successfully, to inhibit the neurons from “burn out” from excessive excitation. Because 90% of folks who have Alzheimers also have the Herpes Simplex-2 Virus, taking a daily antiviral, such as Acyclovir may also be prevention, although not FDA approved for this. Other prescriptions that are used in that AD which by some researchers is considered to be Type 3 Diabetes are Metformine and Actos.
A supplement representing more than 30 years of neuroscience research, is BrainSustain. This is a unique powdered drink formula, developed by Board-Certified Neurologist, David Perlmutter, MD, FACN, to enhance brain performance and health. It is usually given in a smoothie or Almond Milk Shake. BrainSustainTM improves the energy production of brain mitochondria providing generous antioxidant support to combat the damaging effects of excess free radicals. It contains the following underlined ingrediants. Broccoli Seed Extract, which is the Johns Hopkins non heated patented extract of the phytochemical in broccoli (sulforaphane glucosinolate). Extensive research demonstrates that this compound upregulates the Nrf2 system, enhancing the production of important antioxidants such as glutathione and superoxide dismutase as well as activating vital Phase 2 detoxification enzymes. N-Acetyl-L-Cysteine (NAC), a derivative of the amino acid, L-cysteine, is the precursor to glutathione, one of the brain’s most important antioxidants. The aim of oral supplementation is to augment the body’s reserve. NAC itself is a potent antioxidant shown to reduce formation of nitric oxide, a free radical implicated for a causative role in neurodegenerative disorders. Phosphytl Serine (PS), a component of lecithin, plays an important role in neuronal energy production and enhances neuronal communication. After careful examination of scientific evidence, the FDA granted “qualified health claim” status to PS, stating that “Consumption of PS may reduce the risk of dementia in the elderly”. N-Acetyl-L-Carnitine (aka ALCAR), an acetylated form of the amino acid, L-carnitine, is able to cross the blood brain barrier, where it acts as an effective antioxidant and protects brain cells from toxic chemical and stress-induced damage and deterioration. N-Acetyl-L-Carnitine enhances neuronal energy production by transporting fuel sources into the mitochondria and removing energy production waste products from them. Carnitine is readily converted into acetlycholine, a neurotransmittter essential for learning and concentration. Alpha Lipoic Acid also provides more antioxidant action and regenerates other important brain antioxidants including vitamins E, C, and glutathione. Unlike other antioxidants, alpha lipoic acid is both fat and water-soluble, greatly enhancing its ability to be absorbed from the gut and penetrate into the brain. Coenzyme Q10 measurably increases the efficiency of cellular energy production and serves as a potent antioxidant that may protect the brain from oxidative stress damage, which is believed to be partially responsible for neurodegenerative disease. A special DHA, (a2), derived from algae is not only vital to brain health, but 25% of the brain is made up of it. DHA-a2 facilitates optimal structure and functioning of the brain cell membranes.
BrainSustainTM also contains VegaProTM, XYMOGEN’s proprietary pea/ rice protein blend, as well as fat soluble antioxidants, vitamins D3 and E (as mixed tocopherols), and activated B vitamins, including 50 mg of riboflavin and folic acid (as calcium folinate). Available in Vanilla Delight, Chai & Creamy Chocolate, BrainSustainTM costs from $40 to $80 a month depending on whether an individual takes one or two scoops of this product daily. In general I advise one to prevent and two to treat Dementia.
Monday, May 9, 2011
Monday, May 2, 2011
ASPIRIN WORKS
Aspirin is frequently called the “wonder drug” because of its many beneficial properties. Two of the most significant are the prevention of cardiovascular events and cancer. It makes the blood platelets which are 1/10 of the size of a red blood cell less sticky . The drug works by inhibiting the production of prostaglandins forming on the outside membrane of these. Additionally, aspirin induces the formation of Nitric Oxide-radicals an independent mechanism of reducing inflammation in the blood vessels. More recent data also suggests that aspirin modulates signaling through NF-κB, a transcription factor complex, plays a central role in many biological processes, including cancer. This may be why folks who take a low dose aspirin daily for at least five years have a 30% less incidence in breast, prostate, stomach, esophagus, lung, and ovarian cancer. Additionally, if they already have the tumor, have far less distant spread.
Although Hippocrates, in 400 B.C left historical records of treatments, with the mother of aspirin from the bark and leaves of the willow tree, it was not until 1828, that Johann Buchner, professor of pharmacy at the University of Munich, isolated a tiny amount of bitter tasting yellow, needle-like crystals, which he called salicinin and Leroux had extracted salicin, in crystalline form for the first time, and Raffaele Piria succeeded in obtaining the salicylic acid in its pure state. A hundred and fifty years later (1971), British pharmacologist John Robert Vane in London, showed aspirin suppressed the production of prostaglandins and thromboxanes. For this discovery, he was awarded both a Nobel Prize in Physiology and Medicine in 1982 and a knighthood.
More than 50 million people in the U.S. take aspirin every day to help prevent heart attacks, strokes and cancer. However, research has demonstrated that up to 25 percent of these individuals may not benefit from the anti-clotting effect of aspirin, and are more than three times more likely to die from a heart attack or stroke. So Aspirin does not have the same effect on everyone. This suboptimal response to aspirin by an individual is commonly known as aspirin resistance or insensitivity Since these individuals are at increased risk of heart attack or stroke, doctors are beginning to recognize the importance of testing for aspirin effect. On the other hand, the higher doses of aspirin, not only in some will produce a paradoxical clotting effect, but in others a hemorrhage!
Until recently, there was no quick, accurate and effective way to test for aspirin effect. An ADP adhesive study or a specific prostaglandin assay was used in research settings and not paid for by insurances. But now, with the AspirinWorks Test, we can be sure the aspirin is working with a simple no fasting urine test. The AspirinWorks Test is FDA cleared for use in apparently healthy individuals, and test samples can be collected in the doctor’s office at any time. The AspirinWorks Test determines the effect of aspirin on platelets by measuring the level of the biomarker called thromboxane B2 (11dhTxB2). The higher the levels of thromboxane B2, the stickier the blood platelets, and the less impact the aspirin is having. This crucial information allows physicians to individualize a patient’s therapy, which may be as simple as adjusting the dose.
When prescribing blood pressure or cholesterol medication, doctors routinely check the patient’s blood pressure or cholesterol to make sure the patient is getting the right dose of medication. Similarly it is important to know if the dose of aspirin you’re taking is effective. Now, when prescribing aspirin we can then decide to increase or decrease your aspirin dose or if additional medication is needed. As mentioned in my previous writings that just as important is the aspirin to prevent blood from clotting within the blood stream, acetaminophen is needed to inhibit the clot on the arterial wall!
Therefore acetaminophen (Tylenol) has been shown to work in conjunction with the aspirin. At the University of Georgia, Dr. Phillip Greenspan found that the acetaminophen is a potent inhibitor of the enzyme, myeloperoxidase. This enzyme oxidizes the LDL, modifies it in such a way that it is more delectable to the certain white cells (macrophages) that reside within the wall of our arteries. These ingest the LDL cholesterol and cause the plaque and obstruction, which is the father of atherosclerosis. In that the acetaminophen blocks the activity of this enzyme, there is less transformation of the bad cholesterol (LDL) that is available for the macrophages to ingest. This research was presented at the conference on arteriosclerosis, thrombosis and vascular biology in Denver, May 21, 2000 and in 2006 documented by John Merrill PhD at Rutgers. This can also be taken to prevent pain. Some people state it helps them to sleep, when taken at bedtime. Also a recent study at the University of Florida demonstrated that acetamenaphen elevates the mood. The bad press that Acetaminophen has recently had makes this well studied drug almost a curse word. It is true in very high doses like over 6,000 mg a day it can negatively affect the liver and perhaps the kidney, but 1000mg/day is positively healthy for all who want protect their blood vessels.
THE BOTTOM LINE-“Betwixt and between, Aspirin and Tylenol will keep the artery clean” One each 81 mg Aspirin and 500 mg Acetaminophen (TylenolR), both twice a day, will keep the heart attack and stroke away!!
Although Hippocrates, in 400 B.C left historical records of treatments, with the mother of aspirin from the bark and leaves of the willow tree, it was not until 1828, that Johann Buchner, professor of pharmacy at the University of Munich, isolated a tiny amount of bitter tasting yellow, needle-like crystals, which he called salicinin and Leroux had extracted salicin, in crystalline form for the first time, and Raffaele Piria succeeded in obtaining the salicylic acid in its pure state. A hundred and fifty years later (1971), British pharmacologist John Robert Vane in London, showed aspirin suppressed the production of prostaglandins and thromboxanes. For this discovery, he was awarded both a Nobel Prize in Physiology and Medicine in 1982 and a knighthood.
More than 50 million people in the U.S. take aspirin every day to help prevent heart attacks, strokes and cancer. However, research has demonstrated that up to 25 percent of these individuals may not benefit from the anti-clotting effect of aspirin, and are more than three times more likely to die from a heart attack or stroke. So Aspirin does not have the same effect on everyone. This suboptimal response to aspirin by an individual is commonly known as aspirin resistance or insensitivity Since these individuals are at increased risk of heart attack or stroke, doctors are beginning to recognize the importance of testing for aspirin effect. On the other hand, the higher doses of aspirin, not only in some will produce a paradoxical clotting effect, but in others a hemorrhage!
Until recently, there was no quick, accurate and effective way to test for aspirin effect. An ADP adhesive study or a specific prostaglandin assay was used in research settings and not paid for by insurances. But now, with the AspirinWorks Test, we can be sure the aspirin is working with a simple no fasting urine test. The AspirinWorks Test is FDA cleared for use in apparently healthy individuals, and test samples can be collected in the doctor’s office at any time. The AspirinWorks Test determines the effect of aspirin on platelets by measuring the level of the biomarker called thromboxane B2 (11dhTxB2). The higher the levels of thromboxane B2, the stickier the blood platelets, and the less impact the aspirin is having. This crucial information allows physicians to individualize a patient’s therapy, which may be as simple as adjusting the dose.
When prescribing blood pressure or cholesterol medication, doctors routinely check the patient’s blood pressure or cholesterol to make sure the patient is getting the right dose of medication. Similarly it is important to know if the dose of aspirin you’re taking is effective. Now, when prescribing aspirin we can then decide to increase or decrease your aspirin dose or if additional medication is needed. As mentioned in my previous writings that just as important is the aspirin to prevent blood from clotting within the blood stream, acetaminophen is needed to inhibit the clot on the arterial wall!
Therefore acetaminophen (Tylenol) has been shown to work in conjunction with the aspirin. At the University of Georgia, Dr. Phillip Greenspan found that the acetaminophen is a potent inhibitor of the enzyme, myeloperoxidase. This enzyme oxidizes the LDL, modifies it in such a way that it is more delectable to the certain white cells (macrophages) that reside within the wall of our arteries. These ingest the LDL cholesterol and cause the plaque and obstruction, which is the father of atherosclerosis. In that the acetaminophen blocks the activity of this enzyme, there is less transformation of the bad cholesterol (LDL) that is available for the macrophages to ingest. This research was presented at the conference on arteriosclerosis, thrombosis and vascular biology in Denver, May 21, 2000 and in 2006 documented by John Merrill PhD at Rutgers. This can also be taken to prevent pain. Some people state it helps them to sleep, when taken at bedtime. Also a recent study at the University of Florida demonstrated that acetamenaphen elevates the mood. The bad press that Acetaminophen has recently had makes this well studied drug almost a curse word. It is true in very high doses like over 6,000 mg a day it can negatively affect the liver and perhaps the kidney, but 1000mg/day is positively healthy for all who want protect their blood vessels.
THE BOTTOM LINE-“Betwixt and between, Aspirin and Tylenol will keep the artery clean” One each 81 mg Aspirin and 500 mg Acetaminophen (TylenolR), both twice a day, will keep the heart attack and stroke away!!
Tuesday, April 26, 2011
PHYSIOLOGY OF IODINE
A compilation by: W. Robert Doenges, ND
Background:
An excellent source of information regarding iodine historical use in medicine, present day assumptions, sufficiency, safety and physiological implications is available in papers written by Dr. Guy Abraham, Dr Jorge Flechas and Dr. David Brownstein for The Original Internist publication. These papers are available from the web at www.optimox.com. Or a search in Google for the iodine supplement Iodoral will yield the same results.
We encourage the reader to acquaint themselves with the aforementioned papers. A brief summary of their work is included as follows:
History summary:
Swiss physician J.F. Coindet in 1812 had success treating goiter (extreme hypothyroidism) with seaweed and reasoned elemental iodine was the primary reason for his patient’s improvement. He tried tincture of iodine at 250 mg per day with great success in 150 goiter patients. Over the last century physicians refined the iodine compounds until French physician Gene Lugol’s in 1829 devised his formula of 12.5 to 37.5 mg of iodine with potassium iodide in water as the most efficient and sufficient dose. Addition of potassium iodide increased the solubility of iodine sufficiently to be more clinically valuable.
Lugol’s formula was used very successfully until the 1930s for the treatment of hypothyroidism, hyperthyroidism and other medical conditions that demonstrated efficacy. It is noteworthy that only 0.05 mg/day of iodine is necessary to prevent goiter. This amount is available in iodized salt thereby eliminating goiter as a prevalent health concern. However 0.05 mg/day is not enough for optimal health. Iodine is the one halogen (chlorine, bromine and fluorine are the others in order of increasing oxidizing potential) the body requires for many biochemical processes.
History of sufficiency:
In the 1930s physicians started using the recently developed thyroid hormones for treatment of thyroid hypo- or hyper- activity. The assumption was that iodized salt provided iodine sufficiency. Even though the chloride in table salt is a competing halide (chlorine - halogen) there is enough uptake of iodine in iodized salt from the potassium iodide to prevent goiter. Therefore synthetic (patentable) thyroid hormone replacement was developed to increase the thyroid’s production of T4 (thyroxine).
Hintze et al (1) compared the response of patients with simple goiter to administration of I at 400 ug/day and to the administration of T4 at 150 ug/day…. Iodine was more effective by itself than the administration of the T4 hormone by itself.
Most people get iodine in their diet from seafood and iodized salt. However, only about 50% of Americans use iodized salt and because of concerns about high blood pressure, many people have reduced their salt intake. One gram of salt contains 77 mcg of iodine. Because of the high chloride content in table salt, some experts estimate that only about 10% of the iodine in iodized salt is actually absorbed. The recommended daily allowance (RDA) of iodine is 150 mcg (somewhat higher for pregnant women and certain other groups). Though 150 mcg daily may be sufficient to prevent an enlarged thyroid (goiter) and cretinism (severe iodine deficiency in babies leading to mental retardation and impaired development), these values are far short of the optimal values of 12,500 mcg (12.5 mg) recommended by Dr. Abraham. But, even using the lower values, many people still do not get the RDA and tests have shown that the average blood levels of iodine have decreased significantly over the past 30 years, in part no doubt, due to the substitution of bromide for iodide in baked goods in the early 1980’s.
A popular assumption is that physiologic doses of iodine are toxic. In the 1940s a study linked non-radioactive iodine to toxic reactions. It was plainly not true. T4 (thyroxine has 4 iodine atoms) and T3 (triiodothyronine has 3 iodine atoms) are the thyroid’s hormones that are control metabolism. Both have iodine atoms in their molecules. It is obvious that iodine sufficiency is needed for optimal metabolism.
Is there a relationship between iodine and chronic fatigue and other disorders?
Dr. Brownstein writes: “The illnesses that iodine/iodide has helped are many. These conditions include Fibromyalgia, thyroid disorders, chronic fatigue immune deficiency syndrome, autoimmune disorders as well as cancer. Most patients who are deficient in iodine will respond positively to iodine supplementation. In fact, I have come to the conclusion that iodine deficiency sets up the immune system to malfunction which can lead to many of the above disorders developing. Every patient could benefit from a thorough evaluation of their iodine levels.” (2)
Is there a probable relationship to fibrocystic breast disease (FDB)?
Mainland Japanese women have a very low incidence and prevalence of FDB and breast cancer. (13) Several investigators have proposed that the essential element I was the protective factor in mainland Japanese. (4 – 10) If indeed, the essential element I is the postulated protective factor, the administration of I to American women in amounts equivalent to that consumed by mainland Japanese women would be expected to protect them from breast cancer and improve FDB, as previously proposed by Stadel for breast cancer and confirmed for FDB by Ghent et al. (7) Based on data supplied by the Japanese Ministry of Health, the average daily I intake in mainland Japanese is 13.8 mg. (6)
The administration of thyroid hormones to I-deficient women may increase further their risk for breast cancer. In a group of women undergoing mammography for screening purposes (14) the incidence of breast cancer was twice as high in women receiving thyroid medications for hypothyroidism (most likely induced by I deficiency) than women not on thyroid supplement. The mean incidences were 6.2% in controls and 12.1% in women on thyroid hormones. The incidence of breast cancer was twice as high in women on thyroid hormones for more than 15 years (19.5%) compared to those on thyroid hormones for 5 years (10%).
Sodium – iodide symporter:
The ability of the thyroid gland to transport and concentrate iodide from blood is absolutely necessary for the synthesis of thyroid hormones. The key player in this process is the sodium-iodide symporter, an integral membrane protein that resides in the membrane of thyroid epithelial cells. As its name indicates, the sodium-iodide symporter simultaneously transports both Na+ and I- ions from extracellular fluid (i.e. blood) into the thryoid epithelial cell. Considering critical role of iodine trapping in thyroid function, it is not surprising that abnormalities in expression or function of the symporter can lead to thyroid disease.
The sodium-iodide symporter is most highly expressed in thyroid epithelial cells. Lower levels of expression can be detected in mammary gland, salivary gland, stomach and colon, but none of these tissues is known to organify iodide. The presence of the symporter in mammary gland leads to secretion of iodine in milk, which is probably important for thyroid function in neonatal animals. (18 – 22)
One atom of iodine is transported into the cells for every 2 atoms of sodium via the sodium/iodine symporter (NIS). There is also a chloride/iodide symporter called pendrin. Normal saliva/serum iodide ratio is approx. 42. Less than 20 may be due to toxins or very high levels of bromine/fluorine binding to the symporter.
Goitrogens, including
- bromine (from fruit fumigants and processed bakery products)
- chlorine (chloramine byproduct from drinking water chlorination)
- ammonium perchlorate (rocket fuel found in tap water)
- fluorine (naturally occurring in well water plus drinking water fluoridation)
- thiocyanate (from cigarette smoke)
can bind to the NIS (receptor) and damage it preventing iodine from entering the cell. The receptor can possibly be repaired with vitamin C (3000 mg/day) and Celtic (unrefined) sea salt. (16)
The basil membrane of the thyroid cell has the specific ability to pump iodine into the interior of the thyroid cell. This is called Iodide Trapping. In a normal gland the iodine pump concentrates the iodide to about 30 times the concentration in blood. The rate of trapping is influenced by TSH in a negative feedback control method. (17)
Clinical experience:
For clinical experiences the following references are useful.
Fibrocystic Breasts by Jonathan V. Wright, M.D., Published in “Nutrition & Healing” – July 1995
David Brownstein, MD., Iodine. Why You Need It Why You Can’t Live Without It. 2nd Ed. 2006
Saliva iodine significance:
There is ample evidence of renal iodine clearance in the literature in Dr. Abraham’s references and some evidence of salivary uptake from other sources. According to Mr. Zareba under a NASA grant, the mean correlation coefficient ( r ) between iodine elimination for blood/saliva was 0.99, for blood/urine, 0.95, and for saliva/urine, 0.97. The absolute value of iodine concentrations in urine revealed marked variability, which was corrected by adjusting for creatinine levels. (15) That is, with normal symporter there is excellent correlation between the iodine concentration increase in serum and saliva. However, the timing is different.
From Bruger and Member, thyroxine was not concentrated from the blood to saliva but elemental potassium iodide (KI) was from 5 to 7 times that of the blood. The maximal amount of iodine concentrated in the saliva occurred 1 to 2 ½ hours after ingestion of KI peaking to 1200 times the initial salivary iodide. The salivary/blood iodine ratio in the control period was 6 and reached a maximum of 28, 8 hours after ingestion of the iodide. (18) Obviously measuring salivary iodide within several hours of supplementation will result in a very high unusable reading. This effect has been verified by our own tests. Note that normal iodide trapping in the thyroid is about 30 times that in the blood.
Implications:
The hypothesis is that since the salivary iodide uptake from the interstitium and thyroid trapping iodide from the blood is approximately the same order over time, the saliva uptake can be a rough indication of thyroid uptake. If this is true then the saliva/urine ratio can be a rough indication of thyroid iodide sufficiency. There is some anecdotal evidence from non-traditional research to suggest this relationship. Examples are as follows:
J was supplementing Iodoral® (7.5 mg KI + 5 mg Iodine per tab) at the rate of 50 mg/day for nine months (without adverse effect) encouraged by the idea of clearing mercury toxicity (a dental assistant) and tested at 25 PPM saliva and 60 PPM urine iodide. One would expect that after nine months supplementation at this dosage, iodine sufficiency would have been reached. The saliva/urine ratio of
< 1 suggests this conclusion.
Dr. T supplementing for many years with an organic bound iodine in seaweed extract tested 17 PPM saliva and 15 PPM urine. The supplementation will continue but one would expect sufficiency with this long term supplementation. Again the ratio approached 1.
B supplementing 6 months 12.5 mg/day Iodoral® tested 9 PPM saliva and 6 PPM urine suggesting a higher dosage could be used to approach higher residual levels and a lower ratio suggesting sufficiency as not reached. The 24 hour urine iodine loading test would be appropriate.
M was not supplementing but ate substantial amounts of seafood and mostly Mexican foods but very little US produced processed foods. M’s saliva tested 17 PPM and urine 15 PPM.
20 other subjects were tested who were not supplementing except for iodized salt and multivitamin tabs with iodine in the 100 ug range. None were consuming substantial ocean dwelling foods. Usual tests were 1 PPM saliva and 0.1 PPM urine. The absolute values are very low and the ratio is 10. Again a 24 hour urine loading tests would probably support this conclusion.
Testing was performed in the morning with no fast required. It is recommended that a 12 hour fast, 8:00 PM to 8:00 AM for example, be required in order to minimize the effects of hydration.
Future studies
The QFA 1500 analyzer does not purport to provide sensitivities less than 0.1 mg/L (PPM) but is sensitive enough to measure the uptake effects of iodine supplementation whether in Lugol’s formula (as Iodoral® of 7.5 mg potassium iodide and 5 mg elemental iodine) or other organic form such as kelp, dulse or seaweed extract.
The hypothesis of measuring the ratios of saliva vs urine iodine as a measure of sufficiency and blood vs. urine as an indicator of availability of iodine for the tissues (iodine symporter) is unproven except from anecdotal information. Nevertheless a good body of information will be obtained through this simple test coupled with other observation to arrive at conclusions outside traditional expensive and sometimes inaccurate or incomplete medical studies.
References:
1. Hintze, G., Emrich, D., Kobberling, J., Treatment of endemic goitre due to iodine deficiency with iodine, levothyroxine or both: results of a multicentre trial. European Journal of Clinical Investigation, 19:527-534, 1989.
2. Brownstein, D., Clinical experience with inorganic, non-radioactive iodine/iodide. The Original Internist, 12(3):105-108, 2005
3. Eskin B., Bartuska D., Dunn M., Jacob G., Dratman M., Mammary Gland Dysplasia in Iodine Deficiency, JAMA, 200:115-119, 1967.
4. Eskin, B., Iodine Metabolism and Breast Cancer. Trans. New York, Acad. of Sciences, 32:911-947, 1970.
5. Funahashi, H., Imaj, T., Tanaka, Y., et al, Suppressive Effect of Iodine on DMBA-Induced Breast Tumor Growth in the Rat. Journal of Surgical Oncology, 61:209-213, 1996.
6. Ghent, W., Eskin, B., Low, D., Hill, L., Iodine Replacement in Fibrocystic Disease of the Breast, Can. J. Surg., 36:453-460, 1993.
7. Derry, D., Breast Cancer and Iodine, Trafford Publishing, Victoria B.C., 92, 2001.
8. Vishnyakova, V.V., Murav’yeva, N.L., On the Treatment of Dyshormonal Hyperplasia of Mammary Glands, Vestn Akad Med Navk SSSR, 21:19-22, 1966.
9. Cann S., Netten J., Netten C., Hypothesis: Iodine, selenium and the development of breast cancer, Cancer Causes and Control 11:121-127, 2000.
10. Ghandrakant, C., Kapdim MD, Wolfe, J.N., Breast Cancer. Relationship to Thyroid Supplements for Hypothyroidism. JAMA, 238:1124, 1976.
11. Epstein, S.S., Steinman, D., Breast Cancer Prevention Program. Macmillan, NY, 1998, pg 5.
12. Waterhouse, J., Shanmvgakatnam, K., et al, Cancer incidence in five continents. LARC Scientific Publications, International Agency for Research on Cancer, Lyon, France, 1982.
13. Stadel B., Dietary Iodine and Risk of Breast, Endometrial, and Ovarian Cancer, The Lancet, 1:890-891, 1976.
14. Ghandrakant, C., Kapdim MD, Wolfe, J.N., Breast Cancer. Relationship to Thyroid Supplements for Hypothyroidism. JAMA, 238:1124, 1976.
15. Grazyna Zareba, Elsa Cernichiari, Lowell A. Goldsmith, and Thomas W. Clarkson., Biological Monitoring of Iodine, a Water Disinfectant for Long-Term Space Missions. (1) Center for Space Environmental Health, (2) Department of Dermatology, University of Rochester School of Medicine and Dentistry, Rochester, NY 14642 USA, (3) Department of Environmental Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY 14642 USA16.
16. David Brownstein, MD., Iodine. Why You Need It Why You Can’t Live Without It. 2nd Ed. 2006
17. Guyton & Hall, Textbook of Medical Physiology 10th ed.:858, 859)
18. Maurice Berger, Samuel Member, On The Excretion of Iodine in the Saliva, From the Research Laboratory, Department of Medicine, New York Post-Graduate Medical School and Hospital, Columbia University
19. De la Vieja A, Dohan O, Levy O, Carrasco N: Molecular Analysis of the Sodium/Iodide Symporter: Impact on Thyroid and Extrathyroid Pathophysiology. Phys Rev 80:1083-1105, 2000.
20. Dohan O, De la Vieja A, Paroder V, etc: The sodium/iodide symporter (NIS): Characterization, regulation and medical significance. Endocrine Reviews 24:48-77, 2003.
21. Fugiwara H, Tatsumi K, Miki K et al: Congenital hypothyroidism caused by a mutation in the Na+/I- symporter. Nature Genetics 16:124, 1997.
22. Spitzweg C, Heufelder AE: The sodium iodide symporter: its emerging relevance to clinical thyroidology. Europ J Endocrinol 138:374, 1998.
Background:
An excellent source of information regarding iodine historical use in medicine, present day assumptions, sufficiency, safety and physiological implications is available in papers written by Dr. Guy Abraham, Dr Jorge Flechas and Dr. David Brownstein for The Original Internist publication. These papers are available from the web at www.optimox.com. Or a search in Google for the iodine supplement Iodoral will yield the same results.
We encourage the reader to acquaint themselves with the aforementioned papers. A brief summary of their work is included as follows:
History summary:
Swiss physician J.F. Coindet in 1812 had success treating goiter (extreme hypothyroidism) with seaweed and reasoned elemental iodine was the primary reason for his patient’s improvement. He tried tincture of iodine at 250 mg per day with great success in 150 goiter patients. Over the last century physicians refined the iodine compounds until French physician Gene Lugol’s in 1829 devised his formula of 12.5 to 37.5 mg of iodine with potassium iodide in water as the most efficient and sufficient dose. Addition of potassium iodide increased the solubility of iodine sufficiently to be more clinically valuable.
Lugol’s formula was used very successfully until the 1930s for the treatment of hypothyroidism, hyperthyroidism and other medical conditions that demonstrated efficacy. It is noteworthy that only 0.05 mg/day of iodine is necessary to prevent goiter. This amount is available in iodized salt thereby eliminating goiter as a prevalent health concern. However 0.05 mg/day is not enough for optimal health. Iodine is the one halogen (chlorine, bromine and fluorine are the others in order of increasing oxidizing potential) the body requires for many biochemical processes.
History of sufficiency:
In the 1930s physicians started using the recently developed thyroid hormones for treatment of thyroid hypo- or hyper- activity. The assumption was that iodized salt provided iodine sufficiency. Even though the chloride in table salt is a competing halide (chlorine - halogen) there is enough uptake of iodine in iodized salt from the potassium iodide to prevent goiter. Therefore synthetic (patentable) thyroid hormone replacement was developed to increase the thyroid’s production of T4 (thyroxine).
Hintze et al (1) compared the response of patients with simple goiter to administration of I at 400 ug/day and to the administration of T4 at 150 ug/day…. Iodine was more effective by itself than the administration of the T4 hormone by itself.
Most people get iodine in their diet from seafood and iodized salt. However, only about 50% of Americans use iodized salt and because of concerns about high blood pressure, many people have reduced their salt intake. One gram of salt contains 77 mcg of iodine. Because of the high chloride content in table salt, some experts estimate that only about 10% of the iodine in iodized salt is actually absorbed. The recommended daily allowance (RDA) of iodine is 150 mcg (somewhat higher for pregnant women and certain other groups). Though 150 mcg daily may be sufficient to prevent an enlarged thyroid (goiter) and cretinism (severe iodine deficiency in babies leading to mental retardation and impaired development), these values are far short of the optimal values of 12,500 mcg (12.5 mg) recommended by Dr. Abraham. But, even using the lower values, many people still do not get the RDA and tests have shown that the average blood levels of iodine have decreased significantly over the past 30 years, in part no doubt, due to the substitution of bromide for iodide in baked goods in the early 1980’s.
A popular assumption is that physiologic doses of iodine are toxic. In the 1940s a study linked non-radioactive iodine to toxic reactions. It was plainly not true. T4 (thyroxine has 4 iodine atoms) and T3 (triiodothyronine has 3 iodine atoms) are the thyroid’s hormones that are control metabolism. Both have iodine atoms in their molecules. It is obvious that iodine sufficiency is needed for optimal metabolism.
Is there a relationship between iodine and chronic fatigue and other disorders?
Dr. Brownstein writes: “The illnesses that iodine/iodide has helped are many. These conditions include Fibromyalgia, thyroid disorders, chronic fatigue immune deficiency syndrome, autoimmune disorders as well as cancer. Most patients who are deficient in iodine will respond positively to iodine supplementation. In fact, I have come to the conclusion that iodine deficiency sets up the immune system to malfunction which can lead to many of the above disorders developing. Every patient could benefit from a thorough evaluation of their iodine levels.” (2)
Is there a probable relationship to fibrocystic breast disease (FDB)?
Mainland Japanese women have a very low incidence and prevalence of FDB and breast cancer. (13) Several investigators have proposed that the essential element I was the protective factor in mainland Japanese. (4 – 10) If indeed, the essential element I is the postulated protective factor, the administration of I to American women in amounts equivalent to that consumed by mainland Japanese women would be expected to protect them from breast cancer and improve FDB, as previously proposed by Stadel for breast cancer and confirmed for FDB by Ghent et al. (7) Based on data supplied by the Japanese Ministry of Health, the average daily I intake in mainland Japanese is 13.8 mg. (6)
The administration of thyroid hormones to I-deficient women may increase further their risk for breast cancer. In a group of women undergoing mammography for screening purposes (14) the incidence of breast cancer was twice as high in women receiving thyroid medications for hypothyroidism (most likely induced by I deficiency) than women not on thyroid supplement. The mean incidences were 6.2% in controls and 12.1% in women on thyroid hormones. The incidence of breast cancer was twice as high in women on thyroid hormones for more than 15 years (19.5%) compared to those on thyroid hormones for 5 years (10%).
Sodium – iodide symporter:
The ability of the thyroid gland to transport and concentrate iodide from blood is absolutely necessary for the synthesis of thyroid hormones. The key player in this process is the sodium-iodide symporter, an integral membrane protein that resides in the membrane of thyroid epithelial cells. As its name indicates, the sodium-iodide symporter simultaneously transports both Na+ and I- ions from extracellular fluid (i.e. blood) into the thryoid epithelial cell. Considering critical role of iodine trapping in thyroid function, it is not surprising that abnormalities in expression or function of the symporter can lead to thyroid disease.
The sodium-iodide symporter is most highly expressed in thyroid epithelial cells. Lower levels of expression can be detected in mammary gland, salivary gland, stomach and colon, but none of these tissues is known to organify iodide. The presence of the symporter in mammary gland leads to secretion of iodine in milk, which is probably important for thyroid function in neonatal animals. (18 – 22)
One atom of iodine is transported into the cells for every 2 atoms of sodium via the sodium/iodine symporter (NIS). There is also a chloride/iodide symporter called pendrin. Normal saliva/serum iodide ratio is approx. 42. Less than 20 may be due to toxins or very high levels of bromine/fluorine binding to the symporter.
Goitrogens, including
- bromine (from fruit fumigants and processed bakery products)
- chlorine (chloramine byproduct from drinking water chlorination)
- ammonium perchlorate (rocket fuel found in tap water)
- fluorine (naturally occurring in well water plus drinking water fluoridation)
- thiocyanate (from cigarette smoke)
can bind to the NIS (receptor) and damage it preventing iodine from entering the cell. The receptor can possibly be repaired with vitamin C (3000 mg/day) and Celtic (unrefined) sea salt. (16)
The basil membrane of the thyroid cell has the specific ability to pump iodine into the interior of the thyroid cell. This is called Iodide Trapping. In a normal gland the iodine pump concentrates the iodide to about 30 times the concentration in blood. The rate of trapping is influenced by TSH in a negative feedback control method. (17)
Clinical experience:
For clinical experiences the following references are useful.
Fibrocystic Breasts by Jonathan V. Wright, M.D., Published in “Nutrition & Healing” – July 1995
David Brownstein, MD., Iodine. Why You Need It Why You Can’t Live Without It. 2nd Ed. 2006
Saliva iodine significance:
There is ample evidence of renal iodine clearance in the literature in Dr. Abraham’s references and some evidence of salivary uptake from other sources. According to Mr. Zareba under a NASA grant, the mean correlation coefficient ( r ) between iodine elimination for blood/saliva was 0.99, for blood/urine, 0.95, and for saliva/urine, 0.97. The absolute value of iodine concentrations in urine revealed marked variability, which was corrected by adjusting for creatinine levels. (15) That is, with normal symporter there is excellent correlation between the iodine concentration increase in serum and saliva. However, the timing is different.
From Bruger and Member, thyroxine was not concentrated from the blood to saliva but elemental potassium iodide (KI) was from 5 to 7 times that of the blood. The maximal amount of iodine concentrated in the saliva occurred 1 to 2 ½ hours after ingestion of KI peaking to 1200 times the initial salivary iodide. The salivary/blood iodine ratio in the control period was 6 and reached a maximum of 28, 8 hours after ingestion of the iodide. (18) Obviously measuring salivary iodide within several hours of supplementation will result in a very high unusable reading. This effect has been verified by our own tests. Note that normal iodide trapping in the thyroid is about 30 times that in the blood.
Implications:
The hypothesis is that since the salivary iodide uptake from the interstitium and thyroid trapping iodide from the blood is approximately the same order over time, the saliva uptake can be a rough indication of thyroid uptake. If this is true then the saliva/urine ratio can be a rough indication of thyroid iodide sufficiency. There is some anecdotal evidence from non-traditional research to suggest this relationship. Examples are as follows:
J was supplementing Iodoral® (7.5 mg KI + 5 mg Iodine per tab) at the rate of 50 mg/day for nine months (without adverse effect) encouraged by the idea of clearing mercury toxicity (a dental assistant) and tested at 25 PPM saliva and 60 PPM urine iodide. One would expect that after nine months supplementation at this dosage, iodine sufficiency would have been reached. The saliva/urine ratio of
< 1 suggests this conclusion.
Dr. T supplementing for many years with an organic bound iodine in seaweed extract tested 17 PPM saliva and 15 PPM urine. The supplementation will continue but one would expect sufficiency with this long term supplementation. Again the ratio approached 1.
B supplementing 6 months 12.5 mg/day Iodoral® tested 9 PPM saliva and 6 PPM urine suggesting a higher dosage could be used to approach higher residual levels and a lower ratio suggesting sufficiency as not reached. The 24 hour urine iodine loading test would be appropriate.
M was not supplementing but ate substantial amounts of seafood and mostly Mexican foods but very little US produced processed foods. M’s saliva tested 17 PPM and urine 15 PPM.
20 other subjects were tested who were not supplementing except for iodized salt and multivitamin tabs with iodine in the 100 ug range. None were consuming substantial ocean dwelling foods. Usual tests were 1 PPM saliva and 0.1 PPM urine. The absolute values are very low and the ratio is 10. Again a 24 hour urine loading tests would probably support this conclusion.
Testing was performed in the morning with no fast required. It is recommended that a 12 hour fast, 8:00 PM to 8:00 AM for example, be required in order to minimize the effects of hydration.
Future studies
The QFA 1500 analyzer does not purport to provide sensitivities less than 0.1 mg/L (PPM) but is sensitive enough to measure the uptake effects of iodine supplementation whether in Lugol’s formula (as Iodoral® of 7.5 mg potassium iodide and 5 mg elemental iodine) or other organic form such as kelp, dulse or seaweed extract.
The hypothesis of measuring the ratios of saliva vs urine iodine as a measure of sufficiency and blood vs. urine as an indicator of availability of iodine for the tissues (iodine symporter) is unproven except from anecdotal information. Nevertheless a good body of information will be obtained through this simple test coupled with other observation to arrive at conclusions outside traditional expensive and sometimes inaccurate or incomplete medical studies.
References:
1. Hintze, G., Emrich, D., Kobberling, J., Treatment of endemic goitre due to iodine deficiency with iodine, levothyroxine or both: results of a multicentre trial. European Journal of Clinical Investigation, 19:527-534, 1989.
2. Brownstein, D., Clinical experience with inorganic, non-radioactive iodine/iodide. The Original Internist, 12(3):105-108, 2005
3. Eskin B., Bartuska D., Dunn M., Jacob G., Dratman M., Mammary Gland Dysplasia in Iodine Deficiency, JAMA, 200:115-119, 1967.
4. Eskin, B., Iodine Metabolism and Breast Cancer. Trans. New York, Acad. of Sciences, 32:911-947, 1970.
5. Funahashi, H., Imaj, T., Tanaka, Y., et al, Suppressive Effect of Iodine on DMBA-Induced Breast Tumor Growth in the Rat. Journal of Surgical Oncology, 61:209-213, 1996.
6. Ghent, W., Eskin, B., Low, D., Hill, L., Iodine Replacement in Fibrocystic Disease of the Breast, Can. J. Surg., 36:453-460, 1993.
7. Derry, D., Breast Cancer and Iodine, Trafford Publishing, Victoria B.C., 92, 2001.
8. Vishnyakova, V.V., Murav’yeva, N.L., On the Treatment of Dyshormonal Hyperplasia of Mammary Glands, Vestn Akad Med Navk SSSR, 21:19-22, 1966.
9. Cann S., Netten J., Netten C., Hypothesis: Iodine, selenium and the development of breast cancer, Cancer Causes and Control 11:121-127, 2000.
10. Ghandrakant, C., Kapdim MD, Wolfe, J.N., Breast Cancer. Relationship to Thyroid Supplements for Hypothyroidism. JAMA, 238:1124, 1976.
11. Epstein, S.S., Steinman, D., Breast Cancer Prevention Program. Macmillan, NY, 1998, pg 5.
12. Waterhouse, J., Shanmvgakatnam, K., et al, Cancer incidence in five continents. LARC Scientific Publications, International Agency for Research on Cancer, Lyon, France, 1982.
13. Stadel B., Dietary Iodine and Risk of Breast, Endometrial, and Ovarian Cancer, The Lancet, 1:890-891, 1976.
14. Ghandrakant, C., Kapdim MD, Wolfe, J.N., Breast Cancer. Relationship to Thyroid Supplements for Hypothyroidism. JAMA, 238:1124, 1976.
15. Grazyna Zareba, Elsa Cernichiari, Lowell A. Goldsmith, and Thomas W. Clarkson., Biological Monitoring of Iodine, a Water Disinfectant for Long-Term Space Missions. (1) Center for Space Environmental Health, (2) Department of Dermatology, University of Rochester School of Medicine and Dentistry, Rochester, NY 14642 USA, (3) Department of Environmental Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY 14642 USA16.
16. David Brownstein, MD., Iodine. Why You Need It Why You Can’t Live Without It. 2nd Ed. 2006
17. Guyton & Hall, Textbook of Medical Physiology 10th ed.:858, 859)
18. Maurice Berger, Samuel Member, On The Excretion of Iodine in the Saliva, From the Research Laboratory, Department of Medicine, New York Post-Graduate Medical School and Hospital, Columbia University
19. De la Vieja A, Dohan O, Levy O, Carrasco N: Molecular Analysis of the Sodium/Iodide Symporter: Impact on Thyroid and Extrathyroid Pathophysiology. Phys Rev 80:1083-1105, 2000.
20. Dohan O, De la Vieja A, Paroder V, etc: The sodium/iodide symporter (NIS): Characterization, regulation and medical significance. Endocrine Reviews 24:48-77, 2003.
21. Fugiwara H, Tatsumi K, Miki K et al: Congenital hypothyroidism caused by a mutation in the Na+/I- symporter. Nature Genetics 16:124, 1997.
22. Spitzweg C, Heufelder AE: The sodium iodide symporter: its emerging relevance to clinical thyroidology. Europ J Endocrinol 138:374, 1998.
Monday, April 25, 2011
A NOVEL WAY TO TREAT CONNECTIVE TISSUE TRAUMA
CONNECTIVE TISSUE is the supporting structure in a joint including tendons, muscles, ligaments and, in some cases, the cushioning cartilage between the joint. In a person’s life, 100% of us sustain an injury to these tissues. This result in strains and sprains with or without fractures of the involved joint. A strain is an injury to a muscle and/or its tendon, the tissue that connects muscles to bones. A sprain is an injury to a ligament, the tough, fibrous tissue that connects bones to other bone. These injuries involve a stretching or a tearing of the tissue and produces inflammation. “Tendinosis”, a better term than tendonitis, on the other hand refers to non-inflammatory injury to these tissues at the cellular level. These conditions are caused by damage to collagen, cells, and some due to the vascular components of the structure, which ultimately could lead to rupture by a different mechanism than acute trauma. These “tendinopathies” may be caused by both extrinsic and intrinsic factors including age, genetics (Ehlers Danlos Syndrome), body weight and nutrition. The extrinsic factors are often related to sports and include excessive forces or loading, poor training techniques, environmental conditions, posture and gait. Depending on the severity of the injury, the damage may be a simple overstretch of the tissue, or it can result in a partial or complete tear!
A sprain or strain typically occurs when people fall and land on an outstretched arm, slide into base, land on the side of their foot, or twist a knee with the foot planted firmly on the ground. This results in a overstretch or tear of the tendon/muscle or ligament(s) supporting that joint. Strains can be acute or chronic. An acute strain is caused by trauma or an injury such as a blow to the body. Improperly lifting heavy objects or overstressing the muscles can also cause it. Chronic strains are usually the result of overuse injury (prolonged, repetitive movement of the muscles and tendons).
Although all joints can potentially be sprained or strained, the most common is the ankle the second is the shoulder, and the third, the ankle counterpart in the upper extremity, the wrist. The ankle is most commonly severely injured in professional, recreational sports and even in ordinary activities like walking. Most ankle sprains happen when the foot abruptly turns inward (inversion) or outward (aversion) as athletes run, turn, fall, or land after a jump. One or more of the lateral or medial ligaments are injured but a tendon and its attached muscle can also be hurt.
The usual symptom of a muscle/tendon strain or a ligament sprain is pain, and the signs are swelling, bruising, and the loss of function (the inability to move and use the joint). Sometimes people feel a pop or tear when the injury happens. The signs and symptoms can vary in intensity, depending on the severity of the sprain.
The severity is graded one, two and three. A grade I (mild) is overstretching or slight tearing of the tissues with no joint instability. A person usually experiences minimal pain, swelling, and little or no loss of function. Bruising is absent or slight, and the person is usually able to put weight on the affected joint. A grade II (moderate) causes partial tearing and is characterized by bruising, moderate pain, and swelling. There is some difficulty putting weight on the affected joint and there is some loss of function. An x-ray or rarely an MRI may be needed to document both the diagnoses and stage. A grade III (severe) results in a complete tear or rupture. Pain, swelling, and bruising are significant, and the patient is unable to put weight on the joint. An x-ray is usually taken to rule out a fracture in the adjacent bone. Type III injury often requires immobilization and possibly surgery. It can also increase the risk of the person having future problems in that area.
Contact sports such as soccer, football, hockey, boxing, and wrestling put people at risk for strains. Gymnastics, tennis, rowing, golf, and other sports that require extensive gripping can increase the risk of hand and forearm strains. Elbow strains a type of repetitive syndrome occur in people who participate in racket sports, throwing, contact sports and work. The latter in occupations such as carpentry that requires hammering. Two Common Elbow Strains are Tennis Elbow (lateral epicondylitis) and Golfer’s Elbow (medial epicondylitis).
The healing time varies with the severity of the injury with mild and only a few fibers have been damaged. Healing occurs within two to three weeks. With moderate injury with more extensive damage to the fibers, but the tissues is not completely ruptured. Healing occurs within three to six weeks. But with a severe injury and a complete severing of the bundle. It is another story. This may require surgical repair of the tissue and the healing period can be up to a year!
Tendons, muscles, and ligaments are capable of healing and recovering from injuries in a process that is controlled by the fibers and their surrounding extracellular matrix. However, the healed tendons and ligaments never regain the same mechanical properties as before the injury. Muscle have a good blood supply, which is impart why they are red heal far faster and better than the anemic white tendons and ligaments. The three main stages of healing are inflammation, repair ( proliferation), and remodeling. Nature does a good job with these processes, but doctors can help patients to augment the rapidity of healing.
Most current treatments for the joint supportive structures are neither evidence-
based or effective. Typically Doctors recommend RICE- Rest, Ice, Compression, and
Elevation. They also give anti-inflammatory such as Ibuprofen which may help with
the pain, but delays the healing in that inflammation itself as noted above is part of
the healing process. In some cases immobilization may be helpful, but in others in
which there is no associated fracture, it delays healing in that it decreases the
natural growth factors that are stimulated with joint movement.
Molecular processes underlying joint structure healing are now being elucidated.
Metalloproteinase enzymes are thought to have a key role in the regulation of the activity of tendon cells and matrix remodeling in both normal and pathologic structures. The potential roles of neuropeptides, inflammatory mediators and mechanical strain (either too much or too little) acting on the resident tenocytes are noted to stimulate the intrinsic healing G-Proteins. Excessive or inappropriate activity of destructive matrix-degrading enzymes might be a novel therapeutic target for tendinopathy. Tenocytes in the tendon actively synthesize components as well as enzymes such as matrix metalloproteinases . Bone morphogenetic proteins (BMPs) can induce bone and cartilage formation as well as tissue differentiation, and BMP-12 specifically has been shown to influence formation and differentiation of tendon tissue and to promote fibrogenesis.
Now avant guarde physicians give Enzymes such as Bromelain and Papain early in acute trauma, don’t use inflammatory suppressants but pro-inflamants (prolotherapy), early or no immobilization, even irritating the structures such as the “aggravating technique” in tennis elbow, and a cellular level, nitroglycerin (NTG)!
The rational that NTG could be used pharmacologically to accelerate repair in injured tendons has been well documented. Gambito E, "Evidence on the effectiveness of topical nitroglycerin in the treatment of tendinopathies: a systematic review and meta-analysis" (Arch. Phys. Med. Rehabil. 2010;91:1291-305). In a more recent study from the University of Toronto (JAMA.Feb 23;2011) Jamal found that nitroglycerin ointment increased both bone density and strength in postmenopausal women. The mechanism for tendon and bone repair is speculated to be enhancement of a group of connective tissue enzymes, the metalloproteinases and a cytokine, specifically Il-17.
Bearing the above in mind, I have used NTG ointment on over thirty patients with tendon/cartilage injuries to include rotator cuff, hip, knee, and neck with good results. In the past, I have also used a topical muscle relaxant (Flexeral), an antinflamatory (Ketoprofen), an analgesic (Lidocaine) separately or together in an absorptive matrix. I have since added them to NTG to augment the earlier healing liniment and have had even better results. This combination of salubriants must be obtained at a compounding pharmacy. Many medical insurances do pay for these prescription. For more information call Chris Schiller at Economy Pharmacy (918-994-5804).
A sprain or strain typically occurs when people fall and land on an outstretched arm, slide into base, land on the side of their foot, or twist a knee with the foot planted firmly on the ground. This results in a overstretch or tear of the tendon/muscle or ligament(s) supporting that joint. Strains can be acute or chronic. An acute strain is caused by trauma or an injury such as a blow to the body. Improperly lifting heavy objects or overstressing the muscles can also cause it. Chronic strains are usually the result of overuse injury (prolonged, repetitive movement of the muscles and tendons).
Although all joints can potentially be sprained or strained, the most common is the ankle the second is the shoulder, and the third, the ankle counterpart in the upper extremity, the wrist. The ankle is most commonly severely injured in professional, recreational sports and even in ordinary activities like walking. Most ankle sprains happen when the foot abruptly turns inward (inversion) or outward (aversion) as athletes run, turn, fall, or land after a jump. One or more of the lateral or medial ligaments are injured but a tendon and its attached muscle can also be hurt.
The usual symptom of a muscle/tendon strain or a ligament sprain is pain, and the signs are swelling, bruising, and the loss of function (the inability to move and use the joint). Sometimes people feel a pop or tear when the injury happens. The signs and symptoms can vary in intensity, depending on the severity of the sprain.
The severity is graded one, two and three. A grade I (mild) is overstretching or slight tearing of the tissues with no joint instability. A person usually experiences minimal pain, swelling, and little or no loss of function. Bruising is absent or slight, and the person is usually able to put weight on the affected joint. A grade II (moderate) causes partial tearing and is characterized by bruising, moderate pain, and swelling. There is some difficulty putting weight on the affected joint and there is some loss of function. An x-ray or rarely an MRI may be needed to document both the diagnoses and stage. A grade III (severe) results in a complete tear or rupture. Pain, swelling, and bruising are significant, and the patient is unable to put weight on the joint. An x-ray is usually taken to rule out a fracture in the adjacent bone. Type III injury often requires immobilization and possibly surgery. It can also increase the risk of the person having future problems in that area.
Contact sports such as soccer, football, hockey, boxing, and wrestling put people at risk for strains. Gymnastics, tennis, rowing, golf, and other sports that require extensive gripping can increase the risk of hand and forearm strains. Elbow strains a type of repetitive syndrome occur in people who participate in racket sports, throwing, contact sports and work. The latter in occupations such as carpentry that requires hammering. Two Common Elbow Strains are Tennis Elbow (lateral epicondylitis) and Golfer’s Elbow (medial epicondylitis).
The healing time varies with the severity of the injury with mild and only a few fibers have been damaged. Healing occurs within two to three weeks. With moderate injury with more extensive damage to the fibers, but the tissues is not completely ruptured. Healing occurs within three to six weeks. But with a severe injury and a complete severing of the bundle. It is another story. This may require surgical repair of the tissue and the healing period can be up to a year!
Tendons, muscles, and ligaments are capable of healing and recovering from injuries in a process that is controlled by the fibers and their surrounding extracellular matrix. However, the healed tendons and ligaments never regain the same mechanical properties as before the injury. Muscle have a good blood supply, which is impart why they are red heal far faster and better than the anemic white tendons and ligaments. The three main stages of healing are inflammation, repair ( proliferation), and remodeling. Nature does a good job with these processes, but doctors can help patients to augment the rapidity of healing.
Most current treatments for the joint supportive structures are neither evidence-
based or effective. Typically Doctors recommend RICE- Rest, Ice, Compression, and
Elevation. They also give anti-inflammatory such as Ibuprofen which may help with
the pain, but delays the healing in that inflammation itself as noted above is part of
the healing process. In some cases immobilization may be helpful, but in others in
which there is no associated fracture, it delays healing in that it decreases the
natural growth factors that are stimulated with joint movement.
Molecular processes underlying joint structure healing are now being elucidated.
Metalloproteinase enzymes are thought to have a key role in the regulation of the activity of tendon cells and matrix remodeling in both normal and pathologic structures. The potential roles of neuropeptides, inflammatory mediators and mechanical strain (either too much or too little) acting on the resident tenocytes are noted to stimulate the intrinsic healing G-Proteins. Excessive or inappropriate activity of destructive matrix-degrading enzymes might be a novel therapeutic target for tendinopathy. Tenocytes in the tendon actively synthesize components as well as enzymes such as matrix metalloproteinases . Bone morphogenetic proteins (BMPs) can induce bone and cartilage formation as well as tissue differentiation, and BMP-12 specifically has been shown to influence formation and differentiation of tendon tissue and to promote fibrogenesis.
Now avant guarde physicians give Enzymes such as Bromelain and Papain early in acute trauma, don’t use inflammatory suppressants but pro-inflamants (prolotherapy), early or no immobilization, even irritating the structures such as the “aggravating technique” in tennis elbow, and a cellular level, nitroglycerin (NTG)!
The rational that NTG could be used pharmacologically to accelerate repair in injured tendons has been well documented. Gambito E, "Evidence on the effectiveness of topical nitroglycerin in the treatment of tendinopathies: a systematic review and meta-analysis" (Arch. Phys. Med. Rehabil. 2010;91:1291-305). In a more recent study from the University of Toronto (JAMA.Feb 23;2011) Jamal found that nitroglycerin ointment increased both bone density and strength in postmenopausal women. The mechanism for tendon and bone repair is speculated to be enhancement of a group of connective tissue enzymes, the metalloproteinases and a cytokine, specifically Il-17.
Bearing the above in mind, I have used NTG ointment on over thirty patients with tendon/cartilage injuries to include rotator cuff, hip, knee, and neck with good results. In the past, I have also used a topical muscle relaxant (Flexeral), an antinflamatory (Ketoprofen), an analgesic (Lidocaine) separately or together in an absorptive matrix. I have since added them to NTG to augment the earlier healing liniment and have had even better results. This combination of salubriants must be obtained at a compounding pharmacy. Many medical insurances do pay for these prescription. For more information call Chris Schiller at Economy Pharmacy (918-994-5804).
Sunday, April 3, 2011
FOR A LONGER AND BETTER LIFE YOU NEED TO KNOW YOUR SCORE
That score is your telomere count. Although many of us eat and maintain a healthy life style to look and feel better, there is a superior reason. That is to be BETTER and live LONGER. One can be productive and happy as a centurion (living 100+ years). How does one know how long and well they will live? Now there is a laboratory study for it, called TELOMERE TESTING. Until recently, the test was prohibitively expensive, but now for less than $400, one can obtain their report card and intervene on life style to get a better and better score to either achieve their goal or come very close to it. The Telomere test is a simple fasting or non-fasting blood test that can be carried out in most doctor’s office. For more information contact Doug Sloan (405-227 2112) or go on line to Spectocell.com.
Telomeres are sections of DNA at the end of each chromosome whose primary function is to prevent chromosomal “fraying” when a cell replicates. As a cell ages, its telomeres become shorter. How much shorter is governed by genetic factors and environmental stressors. Eventually, the telomeres become too short to allow cell replication, the cell stops dividing and will ultimately die which is a normal biological process. The more of our cells die, the older and frailer we become until we ourselves die. If our reserve is depleted, we succumb to disease or just old age. The Telomere Test can determine the length of your telomeres in relation to the chronological age. The Telomere Score is calculated based on the telomere length on white blood cells (T-lymphocytes). This is the average compared to telomere length on lymphocytes from a sample of the American population of the same age. The higher the telomere score, the “younger” the cells and the longer and better that person will live. Yearly, the test can be repeated and one can work harder or do other interventions that will enhance their score and their life.
Although we cannot change our genes we now can modify their expression by Lifestyle. In a study published in Nature this January scientists found the body activates a gene (P 53) that under stress shuts down our cells' normal growth and division cycle by controlling the telomere length. Diet plays a large role in this process. Micronutrients have been shown to have epigenetic effects by methylation of our DNA. The best but the most difficult is becoming a CRONI, (Caloric Restriction Optimal Nutritional Intake) to the point of just sustenance, a step away from starvation with just nutrient dense foods. Far easier and almost as good is eating correctly for your Apo E type, going easy on meat, with eating whole nutrient dense foods, as raw as possible, consumption of Omega 3s, and staying away from grains and processed foods. According to a study in the January 20, 2010 issue of JAMA, increased telomere and survival rates occurred among individuals with high dietary intake of marine omega-3 fatty acids and established cardiovascular disease. In this 5-year study, the researchers found that individuals with the lowest DHA+EPA experienced the most rapid rate of telomere shortening, whereas those in the highest had the slowest rate of shortening. Levels of DHA+EPA were associated with less telomere shortening before and after sequential adjustment for established risk factors and potential confounders. For each 1-standard deviation increase in red cell Omega 3 levels was associated with a 32 percent reduction in the odds of telomere shortening! Although both EPA and DHA are healthy, it seems that DHA is better. So consuming Tuna or Calamari Oil, which has a 4 to 1 ratio of DHA to EPA, is superior than any of the marine oils. What we eat and supplement today becomes the biology of our future.
Minimizing emotional (psychological) and physiological (infections, trauma and surgery) stress will keep your telomeres longer and you healthier. Additionally, increasing antioxidants slows telomere shortening. Physical exercise with adequate antioxidants will also give longer telomeres. Common sense dictates that decreasing cardiovascular risk factors (Lipids, Homocysteine, Blood Pressure, Hs-C Reactive Protein, Glucose etc.) and correcting micronutrient deficencies such as Vitamins, Minerals, and Glutathione will preserve the telomere length. Periodically getting rid of our poison buildup by colonic, and liver cleanses and from the skin by sweating (artificially by sauna or by heavy exercise) and minimizing the toxins in our water, air and food will go a long way in keeping our telomeres longer. Keeping our hormones (Thyroid, Sex and Adrenal hormones) in balance and not getting sick also keeps our telomeres longer. To not get sick means keeping our immune system healthy to include the consumption of Pre and Probiotics. Surgery should be only for life saving problems and not for elective procedures since the operation and the anesthesia shortens the telomeres. Staying out of harms' way for bodily damage in our daily pursuits such as not over indulging in alcohol and dangerous sports and occupations will keep our telomeres and our lives longer.
Although it is far better to live a healthy life style, there are drugs that also have been shown to decrease our telomere shortening. The antihypertensives, Angiotension Converting Enzyme drugs such as Lisinopril and the Angiotension Recepter Blockers like Lorsartan have been shown to extend our telomeres. Likewise so has the Cholesterol lowering Statins. These drugs should be used judiciously, not to lower our lipids too much and to take concomitantly CoEnzyme Q 10. Also the diabetic medicine, Metformin, has been shown to be antiaging. But with this drug many physicians recommend using B12 too. Age is how old we are, but old is what our body is biologically. In reality it is not how old you are, but how you are when you are old that counts!
Telomeres are sections of DNA at the end of each chromosome whose primary function is to prevent chromosomal “fraying” when a cell replicates. As a cell ages, its telomeres become shorter. How much shorter is governed by genetic factors and environmental stressors. Eventually, the telomeres become too short to allow cell replication, the cell stops dividing and will ultimately die which is a normal biological process. The more of our cells die, the older and frailer we become until we ourselves die. If our reserve is depleted, we succumb to disease or just old age. The Telomere Test can determine the length of your telomeres in relation to the chronological age. The Telomere Score is calculated based on the telomere length on white blood cells (T-lymphocytes). This is the average compared to telomere length on lymphocytes from a sample of the American population of the same age. The higher the telomere score, the “younger” the cells and the longer and better that person will live. Yearly, the test can be repeated and one can work harder or do other interventions that will enhance their score and their life.
Although we cannot change our genes we now can modify their expression by Lifestyle. In a study published in Nature this January scientists found the body activates a gene (P 53) that under stress shuts down our cells' normal growth and division cycle by controlling the telomere length. Diet plays a large role in this process. Micronutrients have been shown to have epigenetic effects by methylation of our DNA. The best but the most difficult is becoming a CRONI, (Caloric Restriction Optimal Nutritional Intake) to the point of just sustenance, a step away from starvation with just nutrient dense foods. Far easier and almost as good is eating correctly for your Apo E type, going easy on meat, with eating whole nutrient dense foods, as raw as possible, consumption of Omega 3s, and staying away from grains and processed foods. According to a study in the January 20, 2010 issue of JAMA, increased telomere and survival rates occurred among individuals with high dietary intake of marine omega-3 fatty acids and established cardiovascular disease. In this 5-year study, the researchers found that individuals with the lowest DHA+EPA experienced the most rapid rate of telomere shortening, whereas those in the highest had the slowest rate of shortening. Levels of DHA+EPA were associated with less telomere shortening before and after sequential adjustment for established risk factors and potential confounders. For each 1-standard deviation increase in red cell Omega 3 levels was associated with a 32 percent reduction in the odds of telomere shortening! Although both EPA and DHA are healthy, it seems that DHA is better. So consuming Tuna or Calamari Oil, which has a 4 to 1 ratio of DHA to EPA, is superior than any of the marine oils. What we eat and supplement today becomes the biology of our future.
Minimizing emotional (psychological) and physiological (infections, trauma and surgery) stress will keep your telomeres longer and you healthier. Additionally, increasing antioxidants slows telomere shortening. Physical exercise with adequate antioxidants will also give longer telomeres. Common sense dictates that decreasing cardiovascular risk factors (Lipids, Homocysteine, Blood Pressure, Hs-C Reactive Protein, Glucose etc.) and correcting micronutrient deficencies such as Vitamins, Minerals, and Glutathione will preserve the telomere length. Periodically getting rid of our poison buildup by colonic, and liver cleanses and from the skin by sweating (artificially by sauna or by heavy exercise) and minimizing the toxins in our water, air and food will go a long way in keeping our telomeres longer. Keeping our hormones (Thyroid, Sex and Adrenal hormones) in balance and not getting sick also keeps our telomeres longer. To not get sick means keeping our immune system healthy to include the consumption of Pre and Probiotics. Surgery should be only for life saving problems and not for elective procedures since the operation and the anesthesia shortens the telomeres. Staying out of harms' way for bodily damage in our daily pursuits such as not over indulging in alcohol and dangerous sports and occupations will keep our telomeres and our lives longer.
Although it is far better to live a healthy life style, there are drugs that also have been shown to decrease our telomere shortening. The antihypertensives, Angiotension Converting Enzyme drugs such as Lisinopril and the Angiotension Recepter Blockers like Lorsartan have been shown to extend our telomeres. Likewise so has the Cholesterol lowering Statins. These drugs should be used judiciously, not to lower our lipids too much and to take concomitantly CoEnzyme Q 10. Also the diabetic medicine, Metformin, has been shown to be antiaging. But with this drug many physicians recommend using B12 too. Age is how old we are, but old is what our body is biologically. In reality it is not how old you are, but how you are when you are old that counts!
Monday, March 7, 2011
CHIROPRACTIC
Nowadays, Chiropractic medicine is an accepted paradigm of health care and treatment. But it was not always like that. Today our society considers these practitioners as in a health care discipline that emphasizes diagnosis, treatment and prevention of mechanical disorders of the vertebrae under the hypothesis that these disorders affect general health via the nervous system. The main chiropractic treatment involves manipulation of the spine, other joints, and soft tissues; treatment also includes exercises and health and lifestyle counseling.
D.D. Palmer founded chiropractic in the 1890s and his son B.J. Palmer helped to expand it in the early 20th century. It has two main groups: "straights", now the minority, emphasize vitalism, innate intelligence and spinal adjustments, and consider vertebral subluxations to be the cause of all disease; "mixers" are more open to mainstream and alternative medical techniques such as exercise, massage, and nutrition. With the advent of X-Ray and the noise of a joint going back into the proper position, Chiropractic is here to stay! The so called pop is caused by the tendons or in the back the apophyseal joint causing a vacuum as it is pulled and suddenly let go-in physics called a cavitation.
The premise of chiropractic assumes a vertebral subluxation or spinal joint dysfunction interferes with the body's function and its Innate Intelligence. This vitalistic concept states that all life contains Innate Intelligence and that this force is responsible for the organization, maintenance and healing of the body. Removal of the interference to the nervous system spinal adjustment so that when the spine is in correct alignment, Innate Intelligence can act, by way of the nervous system, to heal disease within the body. However, until 1987 Chiropractic was considered a cult by the AMA of which I was a member. My experience though with the profession was that it greatly helped folks with back problems and I frequently referred patients to them.
In 1975, I was approached by the Missouri State Medical Board that my license was at stake if I continued using chiropractors as part of the “healing profession”. I was incensed that I could not practice what I thought was best for my patient. Most MDs then thought that if time and physical therapy did not work, then give heavy pain meds or sent them to orthopedic surgeons. Many were operated on and suffered a “failed back”. I was so disturbed by this that I testified in Chicago in 1976, with Chester Wilk and four other chiropractors against the AMA and several nationwide healthcare associations. This was finally resolved in 1987 after a second trial that Chiropratic did help folks indeed and in need.
The triad of Innate Intelligence, Force, and Matter espoused by Palmer a hundred years ago has gone by the wayside. Modern chiropractors study these principles in college and these ideas are seen as historical references to early chiropractic philosophy and pseudoscience. Chiropractors in Australia, England and Germany are Medical Doctors (M.D.s) who specialize in spinal manipulation and many of the techniques used by their American counterparts. A profession that originally did similar healings, the Osteopaths, but now do very little Osteopathic Manipulative Therapy took some of the slack here up. They mostly practice what we as MDs do. After four years of postgraduate (Chiropractic School) training, the student is awarded a Doctorate in Chiropractic- a D.C. Until recently most schools were privately funded, but now they are beginning to see them as part of Universities. Chiropractic is here to stay in America and I feel it is part of the holistic movement of good patient care.
D.D. Palmer founded chiropractic in the 1890s and his son B.J. Palmer helped to expand it in the early 20th century. It has two main groups: "straights", now the minority, emphasize vitalism, innate intelligence and spinal adjustments, and consider vertebral subluxations to be the cause of all disease; "mixers" are more open to mainstream and alternative medical techniques such as exercise, massage, and nutrition. With the advent of X-Ray and the noise of a joint going back into the proper position, Chiropractic is here to stay! The so called pop is caused by the tendons or in the back the apophyseal joint causing a vacuum as it is pulled and suddenly let go-in physics called a cavitation.
The premise of chiropractic assumes a vertebral subluxation or spinal joint dysfunction interferes with the body's function and its Innate Intelligence. This vitalistic concept states that all life contains Innate Intelligence and that this force is responsible for the organization, maintenance and healing of the body. Removal of the interference to the nervous system spinal adjustment so that when the spine is in correct alignment, Innate Intelligence can act, by way of the nervous system, to heal disease within the body. However, until 1987 Chiropractic was considered a cult by the AMA of which I was a member. My experience though with the profession was that it greatly helped folks with back problems and I frequently referred patients to them.
In 1975, I was approached by the Missouri State Medical Board that my license was at stake if I continued using chiropractors as part of the “healing profession”. I was incensed that I could not practice what I thought was best for my patient. Most MDs then thought that if time and physical therapy did not work, then give heavy pain meds or sent them to orthopedic surgeons. Many were operated on and suffered a “failed back”. I was so disturbed by this that I testified in Chicago in 1976, with Chester Wilk and four other chiropractors against the AMA and several nationwide healthcare associations. This was finally resolved in 1987 after a second trial that Chiropratic did help folks indeed and in need.
The triad of Innate Intelligence, Force, and Matter espoused by Palmer a hundred years ago has gone by the wayside. Modern chiropractors study these principles in college and these ideas are seen as historical references to early chiropractic philosophy and pseudoscience. Chiropractors in Australia, England and Germany are Medical Doctors (M.D.s) who specialize in spinal manipulation and many of the techniques used by their American counterparts. A profession that originally did similar healings, the Osteopaths, but now do very little Osteopathic Manipulative Therapy took some of the slack here up. They mostly practice what we as MDs do. After four years of postgraduate (Chiropractic School) training, the student is awarded a Doctorate in Chiropractic- a D.C. Until recently most schools were privately funded, but now they are beginning to see them as part of Universities. Chiropractic is here to stay in America and I feel it is part of the holistic movement of good patient care.
Sunday, February 27, 2011
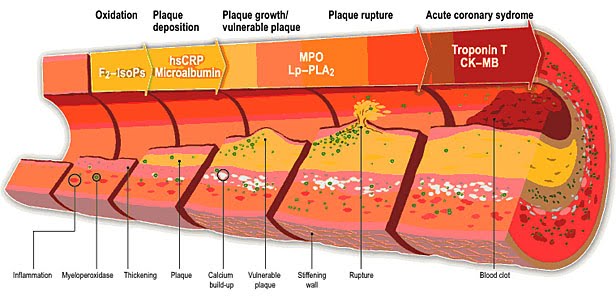
DO YOU KNOW MPO
We all have the enzyme myeloperoxidase, (MPO), in our bodies. But as plaque inside our blood vessel walls becomes more likely to rupture, we produce even more MPO at that site. The increased amounts of MPO, which can be measured in the blood causes erosion of the plaque. When the plaque in the blood vessel erodes enough, it ruptures. There a micro-clot forms to patch the weak spot. Platelets (formed elements) in the blood cells flowing by the clot start participating in growing and firming up this coagulated mass. If that clot blocks blood flow to the heart or brain, a heart attack or stroke usually occurs. A high level of MPO is a signal that a person is in risk of having a catastrophe. This is so even though the cholesterol levels and blood pressure are perfect as in almost fifty percent of these incidents. The MPO oxidizes the LDL cholesterol, modifying so it is more delectable to the certain white cells (macrophages) that reside within the wall of our arteries. These ingest the LDL particles, get sick, die and spill their fatty guts thus enlarging the existing fatty streaks to form an inflammatory plaque. This is the generator of all atherosclerosis. Unbeknownst to most doctors is that Acetaminophen blocks the activity of MPO and stops the transformation of the bad cholesterol (LDL) that is available for the macrophages to ingest.
And Aspirin stops the platelets in our blood from getting sticky, preventing the clump. The basis for the use of low dose aspirin lies in its unique inhibitory effect on a key enzyme, COX-1 (cyclooxygenase-1). In low doses, 81 mg (a child’s aspirin) twice a day, the platelets are less tacky and not as likely to coalesce together to coagulate. However, in higher amounts such as 650 mg (2 adult Aspirins) it affects the arterial walls making them sticky and more likely to initiate a clot on the rough plaque.
A personal friend of mine, Professor Gary Merrill, of Rutgers' department of cell biology and neuroscience, demonstrated significant improvement in acetaminophen-treated hearts compared with non-treated hearts following periods of induced ischemia (reduced blood flow) attributed the rapid post-ischemia recovery of heart muscle and circulation to the antioxidant properties of acetaminophen. This research as part of a growing body of evidence supporting the positive effects of acetaminophen on the cardiovascular system. His findings, together with those of Dr. Addison Taylor of Baylor College of Medicine, Houston, and Professor Phillip Greenspan of the University of Georgia College of Pharmacy, indicate that acetaminophen prevent the damaging effects of LDL cholesterol. Taylor and Greenspan separately conducted investigations showing acetaminophen may protect against the life-threatening condition, hardening of the arteries. The bad press that Acetaminophen has recently had makes this well studied drug almost a curse word. It is true in very high doses like over 6,000 mg a day it can negatively affect the liver and perhaps the kidney, but 1000mg/day is positively healthy for all who want protect their blood vessels.
After the discovery, the Cleveland Clinic, through Cleveland Heart Lab started doing the MPO test. Blood samples, are overnighted to them from the doctors offices, for MPO and four other valuable markers. They include urinary Isoprostain and Microalbumin; a pro-oxidant and an arterial disrupter, HsCRP; indicating lining damage, and Plac2; a predictor of plaque rupture. Many insurance companies and Medicare now cover the test. And for those who don't have coverage, the cost is relatively inexpensive: $189 for MPO and the other tests conducted with it.
If none of the above makes sense to you, still do yourself a favor. Betwixt and between Aspirin and Acetominophen will keep the artery clean-and YOU healthy! If you are a male over the age of 45 or a female over 50-PLEASE take one each of 81 mg Aspirin and 500 mg Acetominophen (Tylenol), both twice a day, it will keep the heart attack and stroke away!!
Subscribe to:
Posts (Atom)